

Do Nsaids Have A Negative Effect On Bone Repair And Recovery After Orthopedic Surgery?
Is Fracture Healing Dumb by NSAIDs?
Written past:Andra Farcas, Dr. (PGY-3) Edited by: Jessica Bode, MD (NUEM 'nineteen) Expert Commentary past: Matthew Levine, Doctor
Clinical Question:
Are nosotros impeding our patients' fracture healing by giving them NSAIDs?
Why is this important?
Broken bones hurt. A lot. And we desire to do something about that to make our patients experience better. In the context of the current opioid crunch and the controversy of prescribing opioids, we need proficient non-opioid alternatives. Enter NSAIDs. Multiple studies have investigated whether nonsteroidal anti-inflammatory drugs (NSAIDs) are efficient pain relievers in multiple scenarios, including fractures, and the consensus seems to lean towards yes. However, this is non a discussion about their effectiveness simply rather an attempt to finally answer the question that emergency docs seem to have different answers to: volition giving patients NSAIDs for their fracture-related pain actually lead to worse outcomes in terms of fracture healing?
Mechanism of action
NSAIDs work by inhibiting the COX enzyme that catalyzes the conversion of arachidonic acid into prostaglandins. In turn, prostaglandins piece of work as inflammatory response mediators. When a bone is fractured, the healing process involves an inflammatory response. Giving NSAIDs alters that inflammatory response by decreasing prostaglandin production. This is why it'due south been proposed that giving NSAIDs to patients with os fractures will bear upon their healing.

Additionally, prostaglandins likewise modify the expression of bone morphogenic proteins (BMPs), which are involved in the os healing process. This is another mechanism by which NSAIDs may affect fracture healing.
What the Research Shows
In that location have been a multitude of brute and human studies investigating the effect of NSAIDs on os fracture healing, mostly in the orthopedic surgery community. The chart beneath has short summaries of some of the ones that are most relevant to emergency medicine.
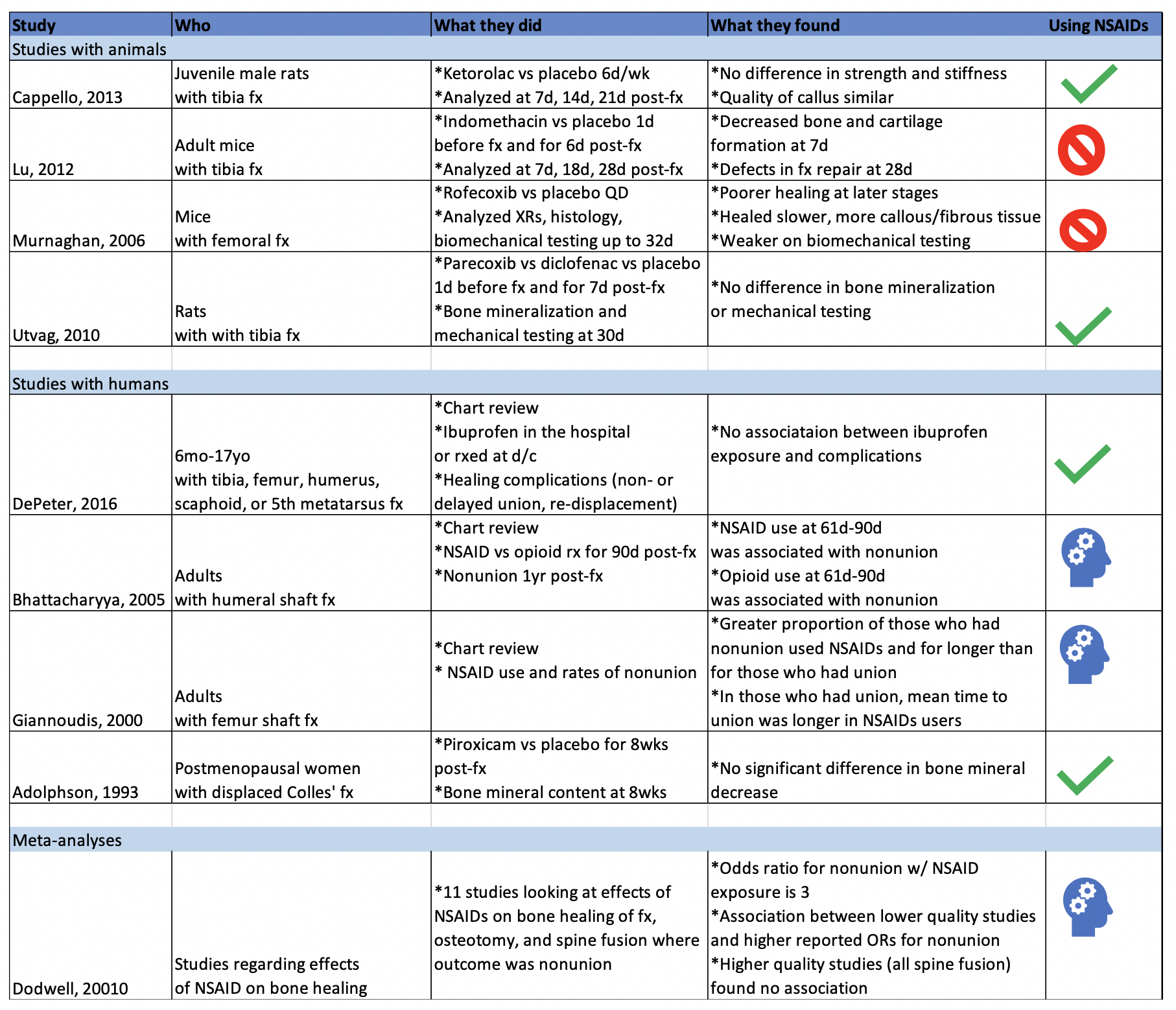
Studies with Animals
Animal studies in general tend to employ mice or rats with induced long bone fractures. The animals are exposed to NSAIDs or placebo and various os characteristics are measured at various fourth dimension frames. Capello, 2022 and Utvag, 2010 showed that Ketorolac, Parecoxib, and Diclofenac had no outcome on strength, stiffness, or bone mineralization in rats with tibia fractures. On the other hand, Lu, 2022 and Murnaghan, 2006 showed that Indomethacin was associated with decreased bone and cartilage formation and that Rofecoxib was associated with slower and poorer healing in mice with tibia and femoral fractures, respectively.
Studies with Humans
While studies with animals accept a lot of advantages, we're often more interested in clinical outcomes than physiological nuances. DePeter 2022 in a retrospective chart review showed no association betwixt ibuprofen exposure in kids with various fractures and healing complications like nonunion, delayed union, or re-displacement. However, there was no specification of the timeframe of treatment, and some patients received ibuprofen in the ED while others were sent domicile with it without a clear defined use period. Adolphson, 1993 showed in that location was no significant difference in bone mineral decrease in postmenopausal women with displaced Colles' fractures that used Piroxicam for 8 weeks after the fracture compared to women who used a placebo. Giannoudis, 2000 institute greater proportion of NSAID use in patients with nonunion of a femur shaft fracture compared to those who had union and establish that in patients who had spousal relationship, those who used NSAIDs took longer to achieve it. Bhattacharyya 2005 found that NSAID use at 61-90 days mail service fracture was associated with nonunion. Nonetheless, an of import thing to point out is that clan does not equal causation. Is information technology that the NSAID apply acquired the poor result? Or is information technology that the poor outcome was more than painful and thus those patients used hurting medication for longer. To that indicate, Bhattacharyya, 2005 also found that at that place was an association between opioid use at 61-ninety days and nonunion.
The Conclusion
The bear witness isn't slam-dunk in either direction on whether using NSAIDs impedes the fracture healing process. There aren't many randomized control trials to explore causation (versus association) of NSAID use with fracture healing outcome. The one RCT I could detect (Adolphson, 1993) leans towards no divergence in outcome between NSAID users and placebo users. My takeaway: if my patients have no other contraindications to using NSAIDs and if their pain is well-controlled with said medication, then I'm going to advise they can utilize it for a brusque term and advise them to seek medical attention if they're still needing to use NSADs regularly a few weeks out.
Good Commentary
As is frequently the case in medicine, confounding factors make seemingly simple questions have non-so-simple answers.
Some animal studies suggested that NSAIDS tin can do harm to healing fractures. Others did not. The benefit of the animal study arroyo is that more than variables can be controlled - the site of fracture, NSAID blazon, dose, frequency, elapsing of therapy. These animals were also surely more compliant with medications and follow upward than our patients. However, creature studies exercise not necessarily translate to man outcomes. And these animal studies were less than definitive anyhow.
The homo studies were also less than definitive. Human studies are difficult for many reasons. Do NSAIDS touch on pediatric, adult, elderly os healing outcomes the same? Does it affair which NSAID, how often it is taken, the dose, the duration of utilise, which bone is fractured? When taking all these factors into consideration, it becomes more clear just how unclear the answer to this question is.
And then at the end of the twenty-four hour period, we do what we do time and time again in medical decision making – a risk-benefit assay:
Pick ane: Give NSAIDS. Risk causing an uncertain NSAID-related complication such as poor os healing or a known NSAID complication such as a cardiovascular/GI/renal issue. Avoid narcotics.
Option 2: Give acetaminophen. Lilliputian downside as long as the patient can follow the directions you requite them or on the bottle to avoid overdosing. Avoid NSAIDS and narcotics.
Pick three: Give narcotics. Avert complications of NSAIDS. Betrayal to complications of narcotics. I don't need to list these.
Option 4: Some combination of options i, 2, and iii because your gestalt is telling you that acetaminophen or NSAIDS alone won't cut it for some cases.
I have different patients that terminate up falling into each of those options. This also raises some other question - how do NSAIDS, acetaminophen, and opiates compare to each other for command of fracture pain? These scenarios and questions again demonstrate that medicine is oft not a robotic ane-size-fits-all, one-answer-to-every-question field, or else Dr. Google would supersede us. Until more definitive RCTs come forth, you will be required to use your judgment, or as I like to telephone call it, expertise.

Matthew Levine, MD
Associate Professor
Section of Emergency Medicine
Northwestern University
How to Cite This Post
[Peer-Reviewed, Web Publication] Farcas A, Bode, J. (2020, April 6). Clinical Question: are we impeding our patients' fracture healing by giving them NSAIDs? [NUEM Web log. Expert Commentary by Levine, 1000]. Retrieved from http://www.nuemblog.com/blog/fx-nsaids
Other Posts You Might Savour…
References
1. Adolphson, P., Abbaszadegan, H., Jonsson, U., Dalen, North., Sjoberg, H.E., Kalen, S. No furnishings of piroxicam on osteopenia and recovery after Colles' fracture: A randomized, double-blind, placebo-controlled prospective trial. Archives of Orthopaedic and Trauma Surgery, 1993; 112: 127-130.
ii. Bhattacharyya, T., Levin, R., Vrahas, M.Southward., Solomon, D.H. Nonsteroidal Antiinflammatory Drugs and Nonunion of Humeral Shaft Fractures. Arthritis & Rheumatism (Arthritis Care & Research), 2005; 53(3): 364-367.
3. Cappello, T., Nuelle, J.A.5., Katsantonis, N., Nauer, R.Chiliad., Lauing, K.L., Jagodzinski, J.Eastward., Callaci, J.J. Ketorolac Administration Does Not Delay Early Fracture Healing in a Juvenile Rat Model: A Pilot Written report. Journal of Pediatric Orthopaedics, 2022; 33(4): 415-421.
4. DePeter, Thousand.C., Blumberg, S.M., Becker, S.D., Meltzer, J.A. Does the utilise of ibuprofen in children with extremity fractures increase their chance for os healing complications? The Journal of Emergency Medicine, 2022; 52(4): 426-432.
5. Dodwell, E.R., Latorre, J.M., Parsini, E., Zwettler, E., Chandra, D., Mulpuri, K., Snyder, B. NSAID Exposure and Risk of Nonunion: A Meta-Assay of Case-Command and Cohort studies. Calcific Tissue International, 2010; 87: 193-202.
6. Giannoudis, P.5., MacDonald, D.A., Matthews, S.J., Smith, R.M., Furlong, A.J., De Boer, P. Nonunion of the femoral diaphysis: the influence of reaming and non-steroidal anti-inflammatory drugs. The Journal of Bone & Joint Surgery, 2000; 82-B(5): 655-658.
7. Lu, C., Xing, Z., Wang, Ten., Mao, J., Marcucio, R.S., Miclau, T. Anti-inflammatory treatment increases angiogenesis during early fracture healing. Artchives of Orthopaedic and Trauma Surgery, 2022; 132: 1205-1213.
8. Murnaghan, M., Li, Grand., Marsh, D.R. Nonsteroidal Anti-Inflammatory Drug-Induced Fracture Nonunion: An Inhibition of Angiogenesis? The Journal of Os and Joint Surgery, 2006; 88-A(iii): 140-147.
nine. Utvag, S.E., Fuskevag, O.M., Shegarfi, H., Reikeras, O. Short-Term Handling with COX-ii Inhibitors Does Not Impair Fracture Healing. Journal of Investigative Surgery, 2010; 23: 257-261.
10. Yates, J.East., Shah, Southward.H., Blackwell, J.C. Do NSAIDs impede fracture healing? The Journal of Family Practice, 2022; threescore(1):41-42.

Do Nsaids Have A Negative Effect On Bone Repair And Recovery After Orthopedic Surgery?,
Source: https://www.nuemblog.com/blog/fx-nsaids
Posted by: monacomourrought.blogspot.com
0 Response to "Do Nsaids Have A Negative Effect On Bone Repair And Recovery After Orthopedic Surgery?"
Post a Comment